This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (http://creativecommons.org/licenses/by-nc/4.0/) which permits unrestricted non-commercial use, distribution, and reproduction in any medium, provided the original work is properly cited.
Evidence-Based Medicine (EBM) demands systematic changes across the healthcare system, essential for enhancing patient safety and quality of medical care. To address the question, "Are we adopting scientific methods to optimize patient safety and enhance treatment efficacy?", assessing the level of EBM implementation is crucial. The adoption rate of evidence-based medical practices varies across countries and medical fields, often being lower in resource-limited settings. In South Korea, there have been several documented cases where the adoption of non-evidence-based practices, such as CARVAR surgical procedures not based on scientific evidence, has led to severe patient safety issues, thereby raising significant concerns about the quality of medical care provided. Conversely, the ABBA Study exemplifies successful application of EBM, demonstrating how scientific research assessed the risk of intracranial hemorrhage in patients with low-dose PPA in OTC cold medicines. This study not only confirmed the associated risks but also influenced health policy, resulting in the withdrawal for PPA-containing OTC cold medicines in Korea. This positive example highlights the imperative for governments, healthcare institutions, and medical schools to expedite the transition to evidence-based, patient-centered healthcare by fostering a robust commitment to systematic reviews and enhanced support for clinical research. The Korean Society of Evidence-Based Medicine (KSEBM) is expected to play a significant role in embedding these core strategies domestically
Evidence-Based Medicine (EBM) emphasizes the importance of scientific evidence in the clinical decision-making process. It has become an essential element in enhancing the quality of healthcare services provided to patients.
The term "evidence-based medicine" was first introduced in 1992 by Gordon Guyatt and Drummond Rennie at McMaster University in Canada, and was later defined by David Sackett in 1996 as "the conscientious, explicit, and judicious use of the current best evidence in making decisions about the care of individual patients." This concept quickly gained global recognition and adoption.
Meanwhile, the World Health Organization (WHO) proposed the concepts of "evidence-informed policy" and "evidence-informed decision making" when emphasizing the importance of utilizing evidence in healthcare policymaking. The WHO stresses that policymaking based on evidence should not be limited to rational execution but must evolve into a deliberative process aimed at achieving fair and reasonable decisions [1].
In Korea, the introduction and advancement of EBM have been driven by the active participation of major public healthcare institutions and medical societies. In 2003, the Health Insurance Review & Assessment Service (HIRA) established the New Health Technology Assessment Team to apply evidence-based decision-making. In 2006, it further launched the Evidence-Based Healthcare Team. Following the 2007 amendment of Article 53 of the Medical Service Act, the New Health Technology Assessment System was legislated, enabling the clinical evaluation of the safety and efficacy of new medical technologies based on EBM principles.
Simultaneously, the Korean Academy of Medical Sciences and the Korean Medical Association developed standardized clinical practice guidelines and, in 2008, founded the Korean Medical Guidelines Information Center(KoMGI). In the same year, the National Evidence-based healthcare Collaborating Agency (NECA) was established, significantly contributing to the development of evidence-based healthcare policies. These efforts have played a crucial role in improving the quality of healthcare in Korea.
In this paper, we aim to outline the necessity and development of evidence-based medicine, introduce practical application cases, and encourage healthcare professionals to recognize the importance of EBM and actively incorporate it into patient care.
Application Level of Evidence-Based Clinical Practice: A Review of Previous Studies
Evidence-Based Medicine (EBM) is a core element for improving the quality of healthcare. Understanding the extent to which EBM is actually applied in various healthcare settings provides critical insight into the necessity for its implementation and the strategic direction for its expansion.
A review of major previous studies indicates that the application rates of EBM in clinical practice vary by country and medical specialty, but generally fall within the range of approximately 70–80%.
In a study conducted by Ellis (1995), it was reported that 82.0% of clinical decisions at a district general hospital in the United Kingdom were based on evidence [2]. Similarly, Gill (1996) reported an application rate of 81.0% at a British teaching hospital, suggesting a relatively high level of EBM practice in primary care settings within the UK [3].
In North America, comparably high application rates have also been observed. Lee JS (2000) reported a 78.0% application rate in the field of thoracic surgery [4], while Khan AT (2006) found a notably high rate of 90.0% in the field of obstetrics and gynecology. In ophthalmology, varying degrees of EBM application have been documented [5]. Lai TYY (2003) reported a 77.0% application rate at an ophthalmology hospital in Hong Kong [6], and Bhatt & Sandramouli (2007) reported an 89.7% application rate in an ophthalmic emergency department in the UK [7]. Despite regional and specialty differences, these findings suggest a relatively stable practice rate of EBM in the ophthalmology field.
Conversely, lower rates have been observed in other settings. Ebell (2017) reported that the EBM application rate in U.S. primary care clinics was 52.0% [8], and Megersa et al. (2023) reported an application rate of 48.4% among nurses working at public hospitals in Ethiopia [9]. These differences likely reflect the influence of multiple factors, including healthcare delivery system characteristics, clinical decision-making autonomy, accessibility to evidence, and the level of professional education (Table 1).
Taken together, these results suggest that the degree of EBM implementation varies depending on the medical specialty, national context, and healthcare infrastructure. In primary care settings and environments with relatively limited resources, the level of EBM practice tends to be lower. This highlights the need for not only the dissemination of guidelines but also the strengthening of healthcare providers' competencies and the provision of structural support to promote the effective implementation of evidence-based medicine.
The Necessity of Introducing Evidence-Based Medicine
The necessity of introducing Evidence-Based Medicine (EBM) extends beyond the mere scientification of clinical practice; it is directly tied to fundamental principles across healthcare, including the protection of patient rights, the enhancement of medical reliability, and the efficient allocation of healthcare resources. Especially as medical care becomes increasingly complex and the range of available treatments expands, establishing objective criteria for determining “the most appropriate treatment” is more critical than ever.
First, EBM serves as an institutional mechanism to safeguard patients' rights to safe and effective treatments. For instance, bariatric surgery for obesity may be effective under specific circumstances, but when performed indiscriminately without established indications or long-term evidence, it can lead to serious adverse outcomes both for individual patients and society at large [10]. Another notable example is the CARVAR (Comprehensive Aortic Root and Valve Repair) surgery, which rapidly spread in Korea during the 2000s without adequate clinical trials, generating significant ethical and medical controversies. This case starkly illustrates the risks associated with medical practices that lack prior scientific validation.
Second, even widely used medical technologies may sometimes be lacking in solid evidence or have uncertain effectiveness. For example, combination analgesic therapies, injection treatments, and repeated imaging studies for functional disorders are routinely employed despite insufficient validation through randomized controlled trials (RCTs). A systematic review evaluating the efficacy of epidural steroid injections for chronic low back pain concluded that their long-term effectiveness in pain reduction was limited [11]. This suggests that the widespread use of a medical intervention does not in itself guarantee its legitimacy.
Third, even when evidence exists, the conclusions drawn from it can vary significantly depending on the quality of the evidence. Arthroscopic surgery for degenerative knee osteoarthritis serves as a prime example: although it was widely practiced for many years, high-quality RCTs later demonstrated no significant difference between arthroscopic surgery and sham surgery, thereby questioning its clinical efficacy [12]. These findings underscore the importance of critically appraising the level of evidence, as high-quality, bias-controlled research can lead to markedly different medical conclusions compared to low-quality studies.
Fourth, there are instances where, despite the existence of strong evidence, clinical adoption was delayed, further highlighting the necessity for EBM. The administration of antenatal corticosteroids to prevent neonatal respiratory distress syndrome was proven effective through RCTs as early as the 1970s [13]. However, it took until the late 1990s for this intervention to be widely adopted in clinical practice due to delays in the dissemination and acceptance of the evidence. Considering the lives of newborns lost to respiratory distress syndrome during that interim period, the critical importance of timely evidence-based adoption cannot be overstated.
Fifth, while the expert judgment of clinicians remains indispensable, decision-making based solely on experience or authority has clear limitations. For example, in the 1970s, Linus Pauling advocated the use of high-dose vitamin C for the treatment of the common cold and cancer [14], yet subsequent large-scale clinical trials demonstrated a lack of scientific support for his claims [15]. This case serves as a cautionary example: even recommendations from prominent authorities can lead to the spread of distorted medical information if they are not grounded in robust scientific evidence.
Finally, in today’s digital era, healthcare professionals face not a shortage of information, but an overabundance. In such an environment, the ability to critically appraise, select, and apply reliable evidence becomes paramount. EBM functions as a systematic tool to evaluate the quality of diverse sources, synthesize findings, and support clinical decision-making amidst a flood of information.
In conclusion, EBM is clearly an indispensable foundation not merely for introducing advanced medical techniques but also for securing the ethicality, efficiency, and credibility of healthcare. In Korea, responding to the increasingly sophisticated demands of the healthcare system requires not only embedding EBM into medical education and clinical practice but also strengthening institutional frameworks. Governmental support for research, guideline development, and implementation strategies must accompany these efforts to firmly establish evidence-based practice across the healthcare system.
Expansion and Evolution of Evidence-Based Medicine: From Concept Formation to the AI Era
Evidence-Based Medicine (EBM), whose necessity is now emphasized more than ever, is not a concept that emerged overnight. Rather, it represents a paradigm that gradually took root through decades of academic discourse and clinical necessity, forming a cornerstone of modern medicine. Especially from the 1980s onward, amid efforts to enhance the scientific validity of healthcare, EBM began to establish its academic identity. In the 21st century, it has entered a new stage through integration with artificial intelligence (AI) and machine learning technologies.
The conceptual foundation of EBM was laid by David Sackett. In his seminal 1981 paper, “How to Read Clinical Journals”, he encouraged healthcare professionals to critically appraise clinical journal articles and integrate the extracted evidence into their clinical decision-making processes [16]. This went beyond merely suggesting a methodology—it proposed the systematic introduction of scientific thinking and critical appraisal principles across all medical practices.
In his 1991 book “Clinical Epidemiology: A Basic Science for Clinical Medicine”, Sackett further defined clinical epidemiology as the "basic science" of clinical medicine, emphasizing the necessity of systematically evaluating and utilizing evidence for diagnosis, treatment, and prognosis [17].
That same year, Guyatt explicitly introduced the term "evidence-based medicine (EBM)", defining it as the integration of clinical expertise, patient values, and the best available external evidence in the decision-making process [18].
Sackett et al.’s classic 1996 paper, “Evidence-Based Medicine: What It Is and What It Isn’t”, provided a clearer articulation of the concept [19]. The authors warned against the misconception of EBM as the mechanical application of randomized controlled trial results. Instead, they framed EBM as a process that integrates an understanding of the individual patient's circumstances and expert’s clinical decision process with the best available scientific evidence. This balanced definition provided both the ethical justification and practical applicability for EBM, facilitating its widespread global adoption.
In his historical overview, Zimerman (2013) characterized EBM as a transformative movement that restructured modern medicine [20]. He analyzed the shift from an authority-centered model of care to an evidence-centered decision-making structure. Similarly, Smith & Rennie (2014) reconstructed the conceptual formation, dissemination, and internal debates of EBM through interviews with key contributors [21]. Their work highlights that EBM did not emerge as a singular academic theory but rather evolved as a body of practical knowledge at the intersection of clinical realities and health policy.
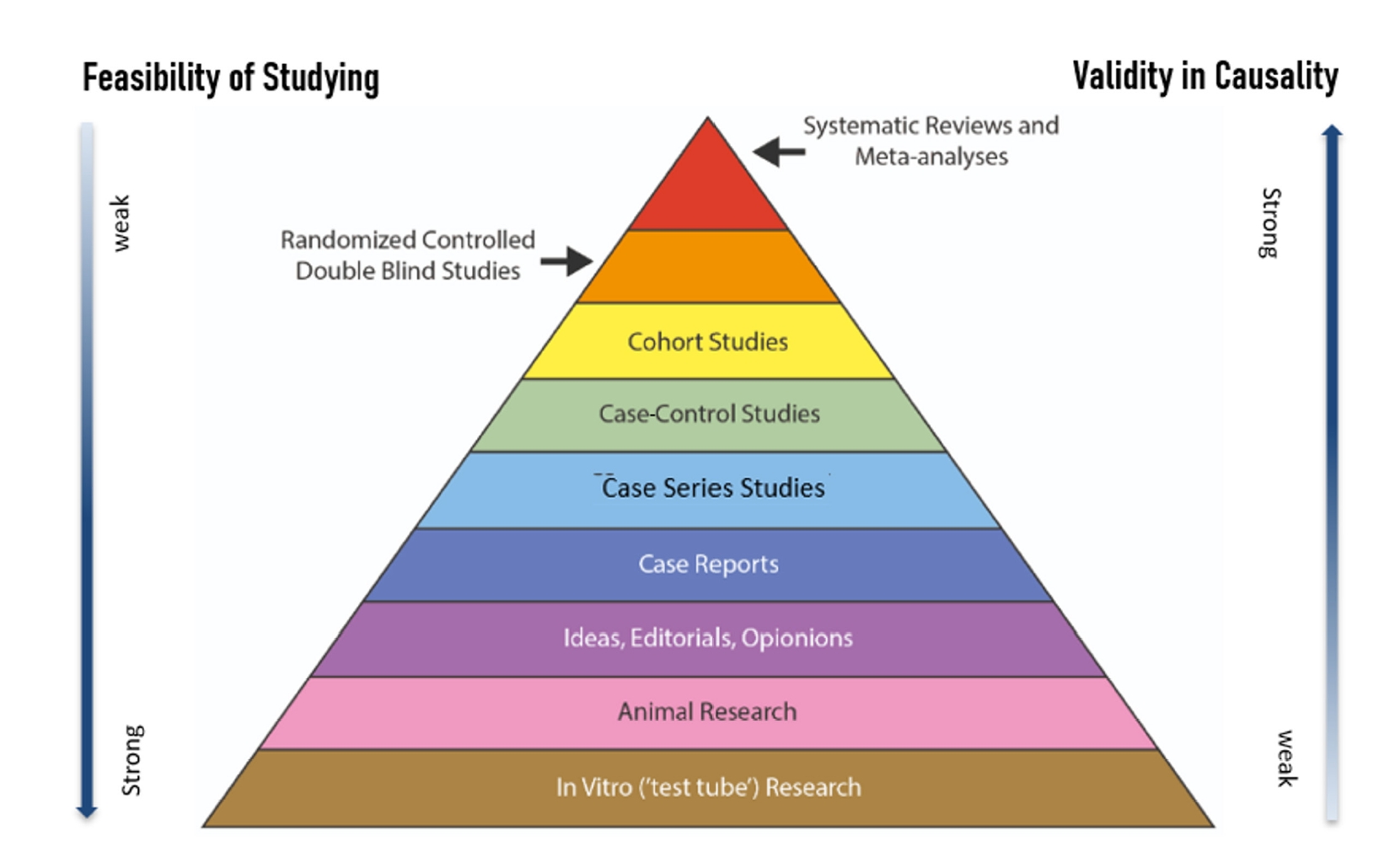
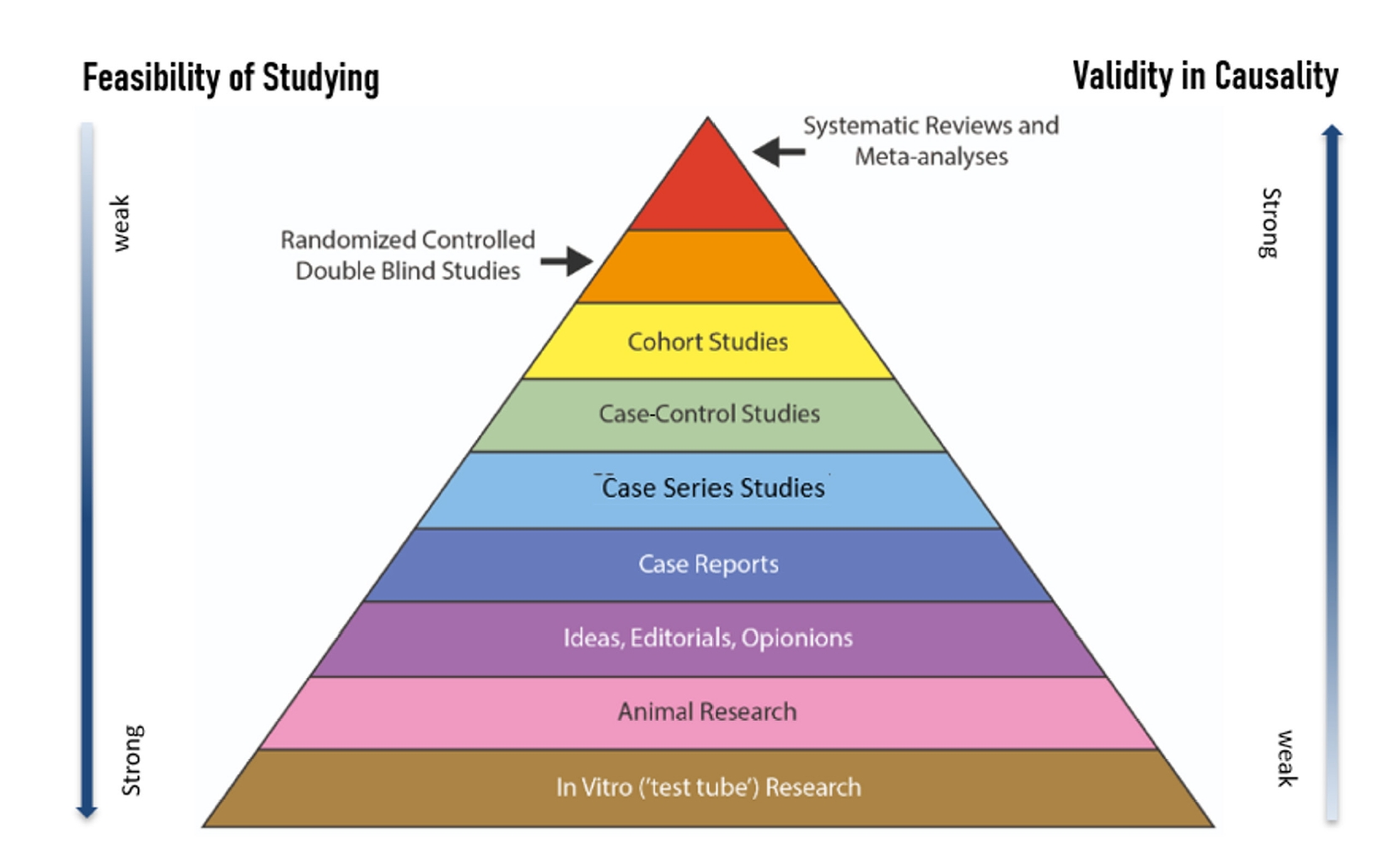
Building on such academic foundations, it became evident that the various types of evidence comprising EBM are organized within a structured hierarchy based on scientific rigor. At the top of this hierarchy are systematic reviews and meta-analyses, followed by randomized controlled trials (RCTs), cohort studies, case-control studies, case series, and case reports.
This classification serves as a framework for assessing the validity and strength of the evidence produced by each study design. Systematic reviews and meta-analyses offer the highest level of persuasive power, providing the most reliable evidence to guide both clinical decision-making and healthcare policy formulation (Fig. 1).
Meanwhile, in the era of artificial intelligence (AI), the hierarchy of evidence based on research design has become even more critical. As data technologies advance, AI contributes to medicine by analyzing large-scale datasets to generate more precise clinical insights.
Chaoyuan Liu et al. (2018) evaluated the accuracy and feasibility of AI-generated treatment recommendations compared to clinical judgments made by physicians for patients with lung cancer in China [22]. This study demonstrated that decision-making processes, which traditionally relied heavily on clinical experience, can now be increasingly structured through AI. Importantly, it opened the possibility for AI to serve not as automatic application, but as a cognitive aid that enhances evidence-based clinical practice without reducing it to mechanical execution.
Moreover, Loughlin et al. (2021) explored how ethical and practical challenges are being redefined in clinical environments where AI and EBM are integrated [23]. They discussed how evidence provided by machine learning systems must harmonize with clinician-patient interactions, value judgments, and contextual interpretations, rather than remaining as mere statistical predictions.
Building on this, McCradden et al. (2025) proposed a comprehensive evaluation framework when applying AI-based clinical decision support systems in pediatric emergency care, addressing not only technical performance but also ethical justification and legal accountability [24].
These developments illustrate that EBM is evolving beyond simply answering “what is the best treatment” to also engaging in deeper philosophical and ethical discussions regarding “how decisions should be made” (Table 2).
In summary, Evidence-Based Medicine does not merely signify the "technologization of medicine." Rather, it represents a transformative journey from decision-making based on experience and authority toward a new clinical culture that integrates scientific evidence with patient-centered values.
Today, this journey is becoming increasingly sophisticated through the incorporation of AI and data-driven technologies, while simultaneously demanding a redefinition of ethical standards.
Amidst these changes, it would be no exaggeration to assert that EBM is evolving from a focus on “how to secure and apply evidence” to a deeper emphasis on “how to derive patient-centered decisions.”
Application of Evidence-Based Medicine in Korean Clinical Practice
Evidence-based medicine (EBM) emphasizes the integration of scientific evidence into clinical decision-making and is increasingly recognized as a core principle for improving patient safety and the quality of healthcare. However, its actual application in Korea shows considerable variability depending on the specific context, and outcomes differ markedly according to the availability of supporting evidence. This section contrasts two representative cases: the CARVAR surgery, introduced without adequate scientific validation, and the ABBA Study, in which systematic evidence generation was directly linked to policy implementation. Through this comparison, we aim to explore the impact of EBM practice on healthcare policy and clinical settings.
CARVAR (Comprehensive Aortic Root and Valve Reconstruction) surgery, a novel type of cardiac procedure involving simultaneous remodeling of the aortic root and valve, attracted attention in Korea as a potential alternative to conventional aortic valve replacement. Advocates claimed it could preserve anatomical structures, maintain physiological function, and avoid long-term anticoagulant use, making it appealing for elderly patients with valvular heart disease [25]. Despite these expectations, CARVAR surgery was introduced into clinical practice without the support of well-designed clinical trials, raising major concerns.
At the time of introduction, only limited animal data regarding safety were available, and no clinical trials had been conducted. By contrast, a similar technique—CAVIAAR, proposed by Emmanuel Lansac—was registered with the U.S. National Institutes of Health (NIH) and was being tested in a multicenter randomized controlled trial [26]. In Korea, however, CARVAR was adopted without even basic information-sharing on such ongoing studies. Following its introduction, no systematic evaluation of patient outcomes or objective technology assessments were performed. Nevertheless, despite concerns over insufficient evidence, the procedure was temporarily approved under conditional non-reimbursement. A retrospective report was later submitted [27], but prospective trials were never undertaken. This case clearly illustrates how applying unverified medical technologies in clinical practice can endanger patient safety, undermine trust in healthcare, and create policy confusion.
In contrast, the ABBA (Acute Brain Bleeding Analysis) Study is widely regarded as a successful example of systematic evidence generation directly influencing national drug regulation. The study was initiated after the U.S. FDA reported that phenylpropanolamine (PPA), previously used as an anti-obesity agent, increased the risk of hemorrhagic stroke. While single-agent formulations were withdrawn in both the U.S. and Korea, the safety of small doses of PPA contained in combination cold medications remained unevaluated in the U.S., prompting a domestic investigation.
From 2002 to 2004, a nationwide prospective case–control study was conducted across 33 hospitals. Patients aged 30–74 years hospitalized for intracerebral or subarachnoid hemorrhage were matched 1:2 with hospital and community controls based on age and sex. Exposure to PPA and potential confounding variables were systematically assessed [28]. Conditional logistic regression revealed that recent PPA use (within 3 days) was associated with a significantly increased risk of hemorrhagic stroke, with an adjusted odds ratio (aOR) of 5.36 (95% CI: 1.40–20.46). Use within 14 days also showed a trend toward increased risk (aOR 2.14, 95% CI: 0.94–4.84), though without statistical significance. The effect was particularly pronounced among women. These findings demonstrated that even small amounts of PPA in cold medications could contribute to hemorrhagic stroke. Based on these results, the Korean Ministry of Food and Drug Safety mandated the withdrawal of all PPA-containing cold medications from the domestic market in August 2004.
The ABBA Study stands as the first large-scale domestic clinical investigation in which evidence directly informed regulatory policy. Its systematic design, nationwide collaboration, and seamless integration from data collection to policy implementation exemplify how evidence generation and policymaking can be effectively linked.
These two contrasting cases demonstrate the transformative role of EBM in healthcare. The CARVAR surgery highlights the risks of adopting new technologies without adequate scientific validation, whereas the ABBA Study illustrates the successful translation of robust evidence into policy action. Together, they provide several key lessons for the Korean healthcare system:
Rigorous Pre-Implementation Validation – All medical technologies must undergo thorough scientific evaluation, ideally through prospective clinical research and institutionalized technology assessment, before adoption.
Evidence-to-Policy Integration – When evidence is established, mechanisms should ensure its timely translation into practical policy, requiring close collaboration between regulators, researchers, and clinicians.
Multidisciplinary and Multicenter Collaboration – Building structural frameworks for large-scale, collaborative research tailored to the Korean population is essential to generate reliable evidence and establish EBM as a functional standard of care.
These lessons underscore that EBM is not merely a theoretical principle but a practical foundation capable of reshaping both clinical practice and healthcare policy.
Conclusion and Recommendations: The Importance of the Korean Society of Evidence-Based Medicine
Evidence-Based Medicine (EBM) has firmly established itself as a core principle for improving the quality of modern healthcare, and its importance is expected to grow even further within Korea’s healthcare system. As technological advances such as artificial intelligence, big data, and precision medicine rapidly transform the medical environment, the ability to critically select and interpret reliable evidence amid a flood of clinical information will become an essential competency.
In particular, as shared decision-making between clinicians and patients becomes increasingly emphasized, EBM is expected to evolve into a standard for more human-centered and ethically grounded medical practice. Furthermore, EBM will occupy a central role in broader areas of public health policy, including the design of data-driven policies and the realization of value-based healthcare systems.
To realize this vision, institutional and structural reforms must accompany these trends.
First, at the governmental level, long-term investment in systematic reviews and clinical research, along with the establishment of comprehensive evaluation systems, is necessary. To accumulate practical evidence directly applicable to clinical practice, it is critical to prioritize research funding allocation and institutionalize evidence-based effect analysis frameworks both before and after the introduction of new technologies. Strengthening information sharing and decision-making coordination among agencies such as the Ministry of Food and Drug Safety, the Ministry of Health and Welfare, and the Health Insurance Review and Assessment Service is also essential to ensure that research findings are effectively reflected in policy.
Healthcare institutions must foster environments that actively support the autonomous practice of EBM. Hospitals should establish infrastructure that enables the planning and execution of clinical research, including dedicated research personnel and data support systems. Additionally, they must develop educational and feedback mechanisms to enhance healthcare professionals’ capabilities in utilizing evidence. EBM must be ingrained into organizational culture as a means to improve not only short-term clinical outcomes but also patient safety and the overall quality of medical care.
Medical schools and health education institutions should firmly establish EBM as a core component of their curricula. Systematic education should encompass methods for conducting systematic reviews and meta-analyses, including hypothesis generation, searching medical literatures relevant to the hypothesis, critical appraisal of the literatures, statistical analysis and interpretation, and integration of clinical judgment with evidence. By nurturing healthcare professionals capable of making evidence-based decisions, EBM can be effectively disseminated across the entire healthcare sector. Furthermore, educational collaborations between tertiary hospitals and primary care facilities should be encouraged to ensure the balanced and widespread adoption of EBM beyond specialized expert groups.
Finally, the Korean Society of Evidence-Based Medicine is expected to play a pivotal role in this transformation. To ensure patient safety, maximize treatment effectiveness, and restore public trust in healthcare, it is essential for EBM to be rapidly and thoroughly embedded into healthcare policy and clinical practice.
The shift in perception, establishment of institutional frameworks, and active initiatives by the Korean Society of Evidence-Based Medicine will not only drive the improvement of healthcare quality but also serve as essential prerequisites for building a sustainable healthcare system in Korea.
3. Gill P, Dowell A, Neal RD, Smith N, Heywood P, Wilson A. Evidence based general practice: a retrospective study of interventions in one training practice. BMJ 1996; 312: 819-21.
5. Khan AT, Mehr MN, Gaynor AM, Bowcock M, Khan KS. Is general inpatient obstetrics and gynaecology evidence-based? A survey of practice with critical review of methodological issues. BMC Womens Health 2006; 6: 5.
6. Lai TY, Wong VW, Leung GM. Is ophthalmology evidence based? A clinical audit of the emergency unit of a regional eye hospital. Br J Ophthalmol 2003; 87: 385-390.
9. Megersa Y, Dechasa A, Shibru A, Mideksa L, Tura MR. Evidence-based practice utilisation and its associated factors among nurses working at public hospitals in West Shoa zone, central Ethiopia: a cross-sectional study. BMJ Open 2023; 13: e063651.
13. Liggins GC, Howie RN. A controlled trial of antepartum glucocorticoid treatment for prevention of the respiratory distress syndrome in premature infants. Pediatrics 1972; 50: 515-25.
14. Cameron E, Pauling L. Supplemental ascorbate in the supportive treatment of cancer: reevaluation of prolongation of survival times in terminal human cancer. Proc Natl Acad Sci USA 1978; 75: 4538-42.
15. Creagan ET, Moertel CG, O'Fallon JR, Schutt AJ, O'Connell MJ, Rubin J, et al. Failure of high-dose vitamin C (ascorbic acid) therapy to benefit patients with advanced cancer. A controlled trial. N Engl J Med 1979; 301: 687-90.
17. Sackett DL, Haynes RB, Guyatt GH, Tugwell P. Clinical epidemiology: a basic science for clinical medicine. 2nd ed. Boston: Little, Brown; 1991. p. 1-20.
18. Guyatt G, Cairns J, Churchill D, Cook D, Haynes B, Hirsh J, et al. Evidence-based medicine: a new approach to teaching the practice of medicine. Ann Intern Med 1991; 114: 253-56.
22. Liu C, Zhu Q, Holroyd KA, Seng EK, Wang Y. Artificial intelligence-based clinical decision support for cancer treatment. J Med Internet Res 2018; 20: e11087.
23. Loughlin M, Copeland SM. Humans, machines and decisions: Clinical reasoning in the age of artificial intelligence, evidence-based medicine and Covid-19. J Eval Clin Pract 2021; 27: 475-77.
24. McCradden MD, Thai K, Assadi A, Tonekaboni S, Stedman I, Joshi S, et al. What makes a 'good' decision with artificial intelligence? A grounded theory study in paediatric care. BMJ Evid Based Med 2025; 12: bmjebm-2024-112919.
26. Lansac E, Di Centa I, Vojacek J, et al. Conservative aortic valve surgery for aortic insufficiency and aneurysms of the aortic root. Clinical Trials. Accessed 2025. Available from: https://clinicaltrials.gov/ct2/show/NCT00478803
27. Bae JM, Shin E, Heo DS. Safety of comprehensive aortic root and valve repair surgery: a retrospective outcomes research by national evidence-based health care collaborating agency, Korea. Korean Circ J 2012; 42: 769-71.
28. Yoon BW, Bae HJ, Hong KS, Lee SM, Park BJ, Yu KH, et al. Phenylpropanolamine contained in cold remedies and risk of hemorrhagic stroke. Neurology 2007; 68: 146-9.